
Okay, so the Mayo docs have relented on the clinic’s policy to the extent that they’re offering me a choice: if I want to take a chance that the 2014 no-ink-on-tumor guidelines for excision margins are safe, they will give me radiation and hormone treatment. Or, if I prefer not to run the 20 percent risk of recurrence and 10 percent risk of invasive cancer, then they will lob off the offending boob.
Which, they wonder, do I prefer?
A man of my acquaintance thinks I don’t understand anything I read on the Internet, especially if the reading level exceeds that of, say, Cosmo or People magazine. I imagine the editor of Mathematical Biosciences and Engineering would disagree, but that’s neither here nor there. Assuming he’s right that I’ve been overthinking this thing, I’ve done a little cost-benefit analysis, based on my subjective feelings about the matter and informed only by facts available in the most dumbed-down sources available to us pretty little air-headed girls.
Interestingly, here’s the result, quite the opposite of the direction in which I’ve been tilting.
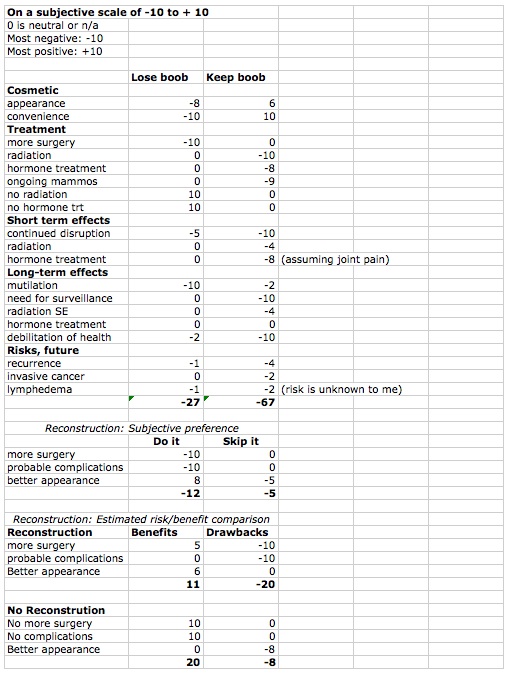 So in this thing, a negative number represents exactly that: a negative. A positive number represents a desirable outcome. A zero indicates either that the circumstance is not applicable or that I don’t care about it one way or the other.
So in this thing, a negative number represents exactly that: a negative. A positive number represents a desirable outcome. A zero indicates either that the circumstance is not applicable or that I don’t care about it one way or the other.
I’ve tried to think of all the aspects entailed in keeping the boob and in having it amputated, and of all the implications entailed in each aspect. Probably I’ve missed some…but I’ll bet I haven’t missed much that matters, at least to me — and this is supposed to reflect my subjective preference.
In terms of whether to keep the boob or not, both options are very negative. We have now heard not one but two heavy-hitting oncologists, both women and at least one of them nationally respected, state that if they personally were faced with this choice, they would try to avoid radiation. I have never reacted well to hormone therapies of any kind, birth control included, and you may be sure that whatever side effects aromatase inhibitors evince, I will be enjoying those. One of them is joint pain. With chronic back pain and sciatica that sometimes flares to the point where I can barely walk down the hall to the bathroom, I don’t feel I need more joint pain. So the fact that each of these therapies has negative side effects, some of them life-threatening, is a bad thing. And even with radiation therapy, the Mayo crew estimates risk of recurrence at 20% and risk of invasive cancer at 10%.
Obviously, the mutilation, the violent surgery, and the ensuing pain of a mastectomy amount to a bad thing, too.
So we’re trying to figure out which is the least bad of two bad options.
And lookit here! Keeping the breast accrues more than twice as many negative points than getting rid of it!
Then we have the fact that these doctors — and one doctor in the wild — are pressuring me to get reconstructive surgery. From what I’ve been able to tell, reconstruction has some failings, most of which result in further surgery or at least disfigurement that you have to learn to live with. Because I am not my boobs, I do not believe that (as one quack informed me) I will quickly become suicidal if I don’t have a fake boob pasted on my chest.
But, just in case I’m staring at this question through a glass darkly, I decided to ask the Excel Ouija board about reconstruction, too. The options presented in my first effort, “Do It” or “Skip It,” seemed a little vague, as it was difficult to know how to score “skip it.” So I tried again with something roughly like a cost/benefit comparison: what are the benefits vs the drawbacks of a) going ahead with reconstruction and b) declining reconstruction?
Here, the result accords more closely with my inclination: the point value of the benefits for no reconstruction outweigh the drawbacks by about three to one. The drawbacks of reconstruction outweigh the benefits by more than three to one. (Would be nice if I’d typed that correctly, but I’m not jumping through the hoops to build and upload a new jpeg for ONE character!)
So. I think this quantifies my point of view on the issue: given two bad choices, the least bad option is mastectomy.
Funny … Ya make me glad I don’t have boobs. What a dilemma….Best of luck in the decision making process.
Don’t get smug, dude! When I remarked to WonderSurgeon that I’d been born into the wrong gender, she squawked “NO!”…and then pointed out that virtually all men develop prostate cancer, if they live long enough.
Here’s what it boils down to: We are all doomed. DOOMED, doomed, doomed. 😮
Honey, sit down and start swilling that wine. 😀
Ha ha! As a matter of fact, that’s exactly what I was doing when that was written… 😉
I’d go with the mastectomy at this point, too. (BTW, your ability to compile and analyze data on just about anything amazes me!)
Sorry if I came across as being smug …. was not my intention. Poor attempt at communicating my angst. I was made aware of the “prostrate curse” when my physician declared that…” you’re either gonna die with it or of it….”….SUPER…
LOL! Ain’t life grand?
Actually, they say that in older men, as with breast cancer in older women, prostate cancer is so slow-moving you’re a lot more likely to die of some other natural cause. Assuming one of our fellow homicidal drivers doesn’t pick us off first…
Oh, man, those homicidal drivers are rampant! The friend I’m staying with through Thanksgiving was in a terrible accident last Friday night. She had a green light and was proceeding straight through an intersection when another driver turned left on a red arrow right in front of her. (Actually, per the damage report the police provided and in looking at the remains of her vehicle, the other driver turned left INTO her.) Her car (which is only four months old) is likely totaled and she was quite banged up (LOTS of bruises and some facial abrasions from the airbags), but thanks to up-to-date safety technology she had no major trauma or broken bones. She is very shaken and does NOT want to drive for a while, and I really don’t blame her. Luckily, I am here with my car and I telecommute with a somewhat flexible schedule, so I can run errands for her and drive her around when needed. (Commuting to work isn’t an issue for her since she gets there via walking and a train, at least.) This is really a life-altering event for her, though. Hopefully, the other driver’s insurance company will pay to replace her (nearly new) car, but she has to get through her fear of getting behind the wheel soon, too.
(Sorry to thread-jack here, but this was a huge event in the past week. I had to pick her up from the accident site and then took her to the ER since she clearly needed care and in her extreme shock declined the ambulance ride. I can’t blog about it because she doesn’t really want to put anything on social media about this herself right now, so I need to hold this in until she breaks the news.)
Oh dear! I’m glad she wasn’t land-in-the-ICU hurt. Friend of mine had something similar happen to her — some clown drove right out in front of her as she was moving through an intersection legally. Totaled her RAV-4 and really banged her up. Fortunately, she also wasn’t hurt enough to spend time in the hospital, but it DID take a long time for her to get over the pain. She apparently had some internal injuries that took quite a while to heal.
And for months she was wary of driving — it made her very nervous to get behind the wheel. Rightfully so, IMHO.
Now on top of the drunks we used to have to dodge and the morons who have always seemed to target us, we have to deal with with idiots who are too busy yakking on the phone or playing with their electronic music media or GPS gadgets to pay attention to where they’re going.
Please, Mr. Google: Get that driverless car on the road ASAP!
Just a thought–you may be overestimating the side effects of the radiation. I was working full time as an accountant when I had my lumpectomy and radiation. I don’t remember feeling tired or any other issues. In fact, what was the most annoying thing was that tape used to map the radiation area took off a layer of skin after being on for 6 weeks. I remember the doc talking about side effects but I had no idea they could occur 30 years later!
That’s not something they tell you. If you knew it, you probably would think twice. Besides, few doctors practice for thirty years, and people move away — a radiation oncologist doesn’t see you for the rest of your life. So from their point of view, their patients appear to be fine. They only see them over a fairly short term.
In my case, though, it appears that the chance of recurrence is pretty high. Do I want to go through radiation and the side effects of five years of aromatase inhibitors? The medical oncologist remarked that not all women tolerate them well; 30% stop taking them before the five years are out. Do I want to go through all this awful surgery AGAIN, only when I’m older and weaker? Heaven help us.
Also, I think when a radiation oncologist says that if it were her, she’d have the mastectomy, she’s tryin’ to tell you something.