So I remain undecided about whether to start taking the calcium-channel blocker (blood-pressure lowering pills) recently prescribed by Cardiodoc. Gut instinct tells me not to do this! But of course, Cardiodoc is a doctor, and I was brought up by a mother who believed with all her heart that doctor knows best.
So I remain undecided about whether to start taking the calcium-channel blocker (blood-pressure lowering pills) recently prescribed by Cardiodoc. Gut instinct tells me not to do this! But of course, Cardiodoc is a doctor, and I was brought up by a mother who believed with all her heart that doctor knows best.
In her case, he didn’t…but that’s another story, hm?
Moving on, here is the basis of my skepticism: In 2016 a six-year randomized study of 12,705 patients (published in the New England Journal of Medicine and widely known as the Hope-3 study) showed that the use of blood pressure medications (such as calcium-channel blockers) indeed did lower blood pressure, but that among people with only moderately elevated blood pressure, they did not reduce the incidence of strokes and cardiovascular events compared, over time, with the control group whose members were given a placebo. The use of statins did show a positive benefit in this group, which did not vary by LDL level or risk level.
The evidence is clearest [we are told] in the cholesterol-lowering arm of the trial. For the intermediate risk population tested in HOPE-3, the trial adds to the large amount of “clear evidence” showing the benefit of statins, said Yusuf. In sharp contrast, the blood pressure arm did not find any overall benefit for antihypertensive therapy, though there was a benefit in the prespecified subgroup with the highest blood pressure levels. The benefits of statins, on the other hand, did not vary by LDL level or level of risk.
Results in the blood pressure arm were more complicated. Overall there was no significant difference in clinical outcomes, but there were significant differences based on the prespecified subgroups of blood pressure at baseline. Trial patients with the highest third of blood pressure at baseline (above 143 mm Hg) derived benefit from antihypertensive therapy. For patients in the middle third, antihypertensive therapy had a neutral effect. For patients in the lowest third, antihypertensive therapy had a harmful effect. [My emphasis.]
So what WERE the middle third, first third, bottom third??
The average blood pressure at baseline for the study participants was 138/82 mm Hg. The authors describe “patients who truly had hypertension” as those with systolic pressure of more than 143.5 mm Hg. I’m not finding explicit figures delineating these groups in the published study; however, the Mayo Clinic lists these:
- Normal blood pressure. Your blood pressure is normal if it’s below 120/80 mm Hg.
- Elevated blood pressure. Elevated blood pressure is a systolic pressure ranging from 120 to 129 mm Hg and a diastolic pressure below 80 mm Hg. Elevated blood pressure tends to get worse over time unless steps are taken to control blood pressure.
- Stage 1 hypertension. Stage 1 hypertension is a systolic pressure ranging from 130 to 139 mm Hg or a diastolic pressure ranging from 80 to 89 mm Hg.
- Stage 2 hypertension. More severe hypertension, stage 2 hypertension is a systolic pressure of 140 mm Hg or higher or a diastolic pressure of 90 mm Hg or higher.
Depending on the time span, you could place me in the Stage 1 category (in December 2017 my average figures for the month were 132.5/83.3) or in the “Elevated” category (between June 2017 and today, my average blood pressure has been 128.1/77.5). I can push the systolic figure down by 6 or 8 points simply by doing a 20-minute yoga routine or by performing five minutes of deep-breathing exercises. This presumably would put me in the “middle third” of the Hope-3 study’s subjects, most of the time and in the lower third (120-128/<80) some of the time.
Apparently, what the HOPE-3 researchers regard as “intermediate” is significantly higher than that. We have this from them (NEJM):
Observational studies involving persons without cardiovascular disease show a graded increase in risk at systolic blood-pres sure levels above 115 mm Hg. It has been suggested that lowering blood pressure at any level above this value will reduce the risk of cardiovascular events. . . . However, the role of therapy in persons at intermediate risk (defined as an annual risk of major cardiovascular events of approximately 1%) who do not have vascular disease and who have a systolic blood pressure of less than 160 mm Hg (who represent the majority of middle-aged and older persons) remains less clear. We evaluated this question in the HeartOutcomes Prevention Evaluation (HOPE)–3 trial. [My emphasis.]
IMHO, 1 percent per year is not a very high risk. After 20 years, that would give you about a 20% chance of a stroke or cardiac event. Since most women would start to see this elevation in their 60s, they’d be their 80s before they had a one-in-five chance of an incident. No, 20% is not great. One would prefer better odds. But it’s not an extremely high risk, either.
So what does this mean in real life? For practicing physicians and their patients?
At last we are able to cite reliable ball-park figures from a representative population at intermediate risk of cardiovascular disease. They confirm that statins reduce risk by about a quarter, whatever the starting point, whereas for blood pressure lowering below a systolic of 143, this does not appear to be true over 5-6 years. However, it may be that BP lowering has benefits over a longer period of time, particularly for the risk of heart failure. [My emphasis.]
And further:
However, treating those with lower blood pressure with the combination is not justifiable. Only statins should be used for them, [said Dr. Eva Lonn, one of the researchers; my emphasis.]
Statins have fewer side effects than blood-pressure-lowering medications. In the Hope-3 study, many fewer people discontinued them than those who discontinued antihypertensives. Neverthless, these treatments may be associated with one dreaded side effect: “Cognitive decline was noted in all patients. The primary outcome, processing speed (measured by Digit Symbol Substitution Test [DSST] at study end) for rosuvastatin vs. placebo: 29.1 vs. 29.4 (p = 0.38); for BP lowering vs. placebo: 29.1 vs. 29.4 (p = 0.86); for combination vs. placebo: 29.3 vs. 29.9 (p = 0.63). Any functional impairment for rosuvastatin vs. placebo: 57% vs. 59%, p = 0.89; for BP lowering vs. placebo: 59% vs. 56%, p = 0.19.” [My emphasis.] Appears to be about the same for either class of drug…since many of the subjects were in their 70s, this effect could simply be age-related.
So, the new American Heart Association guidelines make these recommendations:
- Only prescribing medication for Stage I hypertension if a patient has already had a cardiovascular event such as a heart attack or stroke, or is at high risk of heart attack or stroke based on age, the presence of diabetes mellitus, chronic kidney disease or calculation of atherosclerotic risk (using the same risk calculator used in evaluating high cholesterol).
- Recognizing that many people will need two or more types of medications to control their blood pressure, and that people may take their pills more consistently if multiple medications are combined into a single pill.
So if you believe this, I should be on a statin, not on a BP lowering med. Okay, fine…so what is this stuff I have in this bottle of pills here?
The stuff Cardiodoc prescribed, amlodipine besylate, is a calcium-channel blocker, an antihypertensive. It most commonly gifts you with these fine effects:
Y’know…the last time a cardiodoc inflicted one of these drugs on me, it caused such extravagant vertigo that it became unsafe for me to drive my car. And look at this: it causes palpitations: the very symptom that drove me to seek a doctor in the first place!
We now have determined that my underlying vertigo complaint probably results from inner-ear congestion, which itself probably results from chronic sinus congestion caused by living with two furry dogs in a climate most richly characterized by airborne dust.
The main negative side effect of statins is cataracts. Most people will get cataracts anyway, should we live long enough. Thus I don’t see that as a deal-killer.
But dizziness that could cause me to fall on the hard tile floors or crash my car? Fatigue, swelling of legs and ankles, heart arrhythmia or palpitations, tremors? Yeah, those are deal-killers, in the present circumstances.
Those circumstances being a) it’s unclear that my blood pressure is high enough to justify treatment with drugs at all; and b) the Powers That Be are now recommending a different class of drugs.
Why is the guy not following AHA guidelines? Is his knowledge out of date? Has something new been reported that I’m not finding? Unknown…but in the absence of other data, I am very skeptical about taking this stuff. I just do not need to cope with another raft of nasty side effects.
A Different Strategy…or Gaming the BP Monitor?
Interestingly, I learned from a friend that you can push your blood pressure readings down by doing some deep-breathing for about three minutes before the machine is turned on.
The day before yesterday I tried this. I’d just raced in the door from a particularly exasperating drive through a round of frustrating and annoying errands. Before even putting anything away, I instantly attached the BP cuff and ran the machine (you’re supposed to sit quietly without moving or speaking for about five minutes before running a test). The result was blood-curdling: 149/93.
Cripes! I should be dead!
Now I do a series of deep, diaphragmatic breaths, as learned from LaMaze and voice classes. After five minutes of this and another minute of normal breathing, I try again…and get a 19-point drop in blood-pressure reading!
Holy crap!
Well, obviously that’s too bizarre to put much stock in.
Restarting minutes later, though, the Omron (which was just checked against Cardiodoc’s machine) showed three consistent measures in a row of 130/86, 131/89, and 131/89.
That is still 18 points below the height to which driving in Phoenix traffic had just driven my blood pressure.
Ohhhkayyyy… Let’s try that again after the dust settles. An hour later, the machine produced these results:
120/77, pulse 84
124/72, p. 87
116/72, p. 84
Average of the three readings: 120/74, p. 85
And that, folks, ain’t bad for an old bat who’s pushing 73.
Yesterday, I decided to see what would appear after a 20-minute yoga routine. And what did that elicit?
130/83, p. 87
121/77, p. 87
117/78, p. 87
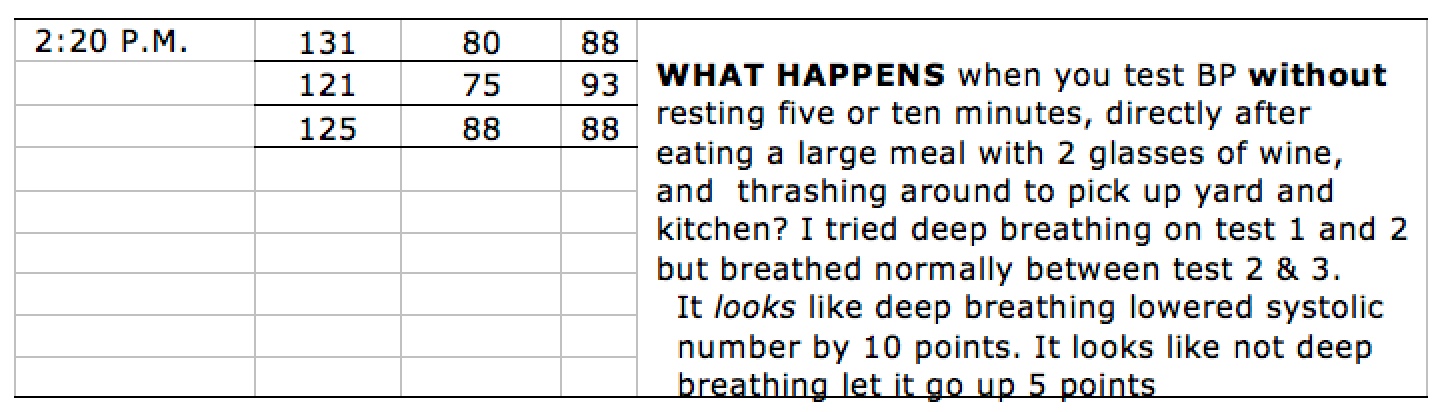
This, after a full meal, 2½ glasses of wine, and a fistful of chocolate chips. The belly was uncomfortably full…and that should push one’s BP figures up markedly.
So what happens if you test after yoga, on an empty stomach? This morning we have the results, obtained while the dogs were hassling around and I was in a rush to get out of the house for a dental appointment:
117/85, p. 84
117/84, p. 79
113/80, p. 77
Doesn’t look like I’m gonna keel over dead very soon, does it?
So I’m not sure what to make of this.
Is it credible, or is it really just a form of gaming the machine? If you did yoga on a regular basis — at least once a day, or maybe even two or three times a day, would your blood pressure drop into the “mildly elevated” or into the “normal” range and stay there most of the time, barring any enraging events?
That, I do not yet know. Yesterday, when the yoga routine was followed by a whole lot of food, readings remained in the “mildly elevated” region a few hours later: average was 126/83.
Today I was unable to test the status after a round-trip to the dentist’s office, an hour in the chair getting my teeth cleaned, and a side-trip to a grocery store, because the minute I sat down to run the Omron machine, a worker showed up at the front door. That person is still here working on a series of minor maintenance tasks, and so it will be another hour or two before I can see what the story is. By then I probably will have had something to eat, which will skew the results some. I guess.
If eating skews results, are the results real?
If deep breathing skews the results, are the results real?
If a short yoga routine skews the results, are the results real?
Those, in my none-too-humble opinion, are the kinds of question that cast doubt on this whole already doubtful affair.
First, it’s doubtful whether the doctors themselves know whether subjecting middle-aged and elder adults to expensive medication (one jar of this stuff goes for $125!!!) does any good. Some researchers think that for some categories of such adults drugging does no good and so (because of the inevitable side effects) actually does harm. And research has shown that one class of drugs, while it does push the numbers down, does exactly nothing to decrease mortality and morbidity rates.
Meanwhile, if you’re looking for something to focus on for your meditation: consider the enormity of the profit that can result from putting every aging Baby-Boomer on drugs that cost $125 a bottle.
Who, really, benefits from this?
Still undecided, then, whether to start gulping these pills.
But my sense is, as usual…
When in doubt, don’t.

 Exactly one week ago I decided that enough was enough with the blood pressure conundrum. By this time last week, I had myself so worked up that I was spiking 150/97 readings(!!) and feeling just like you feel when you have to make a cold call and tell or ask some total stranger something, or like you feel in the 6th grade when you’re about to take a math or spelling quiz. At length I realized that the tension caused by obsessing over this bullshit simply had to be what is pushing up those crazy, never-before-seen spikes.
Exactly one week ago I decided that enough was enough with the blood pressure conundrum. By this time last week, I had myself so worked up that I was spiking 150/97 readings(!!) and feeling just like you feel when you have to make a cold call and tell or ask some total stranger something, or like you feel in the 6th grade when you’re about to take a math or spelling quiz. At length I realized that the tension caused by obsessing over this bullshit simply had to be what is pushing up those crazy, never-before-seen spikes. Three days into said project, along came…amazing! an ocular migraine! Sumbeach! A pair of pinking shears meandering across the field of vision… Who’d’ve thunk it?
Three days into said project, along came…amazing! an ocular migraine! Sumbeach! A pair of pinking shears meandering across the field of vision… Who’d’ve thunk it?